
[box type=”bio”] Learning Point for this Article: [/box]
Aneurysmal Bone Cyst in metacarpal is a rare finding and good radiological and clinical outcome can be achieved by adequate curettage and bone grafting.
Case Report | Volume 8 | Issue 2 | JOCR Mar – Apr 2018 | Page 9-12| Saurav Narayan Nanda, Sanjay Tripathi, Shaikh Muzammil Shiraz, Sudhir Warrier. DOI: 10.13107/jocr.2250-0685.1024
Authors: Saurav Narayan Nanda[1], Sanjay Tripathi[1], Shaikh Muzammil Shiraz[1], Sudhir Warrier[2]
[1]Resident, Department of Orthopaedics & Trauma, Lilavati Hospital and Research Centre Mumbai, Maharashtra, India.
[2]Consultant Orthopaedic Hand Surgeon, Lilavati Hospital and Research Centre Mumbai, Maharashtra, India
Address of Correspondence:
Dr. Saurav Narayan Nanda,
Department of Orthopaedics &Trauma, Lilavati Hospital and Research Centre Mumbai, Maharashtra, India.
E-mail: saurav.scb@gmail.com
Abstract
Introduction: Aneurysmal bone cysts of the hand are rare, and only few cases are reported in scientific literature. We report a case of aneurysmal bone cyst of 3rd metacarpal treated at our tertiary care hospital, Mumbai.
Case Report: A 13-year-old young female presented with pain and progressive increase in swelling over the dorsum of the right hand for 7–8 months. There was pain and tenderness over 3rd metacarpal. There was painful restriction of movement at the metacarpophalangeal joints. Serial radiographic evaluation of the hand from May 2009 to October 2010 showed multilocular expansile lytic lesion with ballooning of 3rd metacarpal with increasing size. The patient was managed surgically with bone grafting. Histopathology section suggested fibrous septa enclosing hemorrhagic cystic space. Septa contained bony chips, spindle cell, inflammatory cell, and few scattered osteoclast. Diagnosis of aneurysmal bone cyst of 3rd metacarpal was made. The patient was followed up after 5 years with good radiological healing with pain-free and good range of motion, good grip strength without any recurrence.
Conclusion: Aneurysmal bone cyst is a rare, rapidly growing, and destructive benign bone tumor. Many treatment modalities have been reported in literature including radiation, curettage and bone grafting, cryotherapy, and excision. However, controversy exists in the literature regarding optimal treatment. Due to its rarity in the hand, no evidence-based treatment regimen has been established. The patient can be managed surgically with bone grafting with good radiological healing with pain-free and good range of motion, good grip strength without any recurrence.
Keywords: Aneurysmal bone cyst, metacarpal, benign bone tumor.
Introduction
Aneurysmal bone cyst is a rare, rapidly growing, and destructive benign bone tumor. It rarely involves the bones of the hand. Aneurysmal bone cyst accounts for 5% of all primary bone tumors. The majority of primary lesion develops in the spine and the long bones of the lower extremity, and 18% involves the upper extremity with 3–5% involving the hand and wrist [1,2]. Aneurysmal bone cyst was first described by Jaffe and Lichtenstein in 1942. Aneurysmal bone cyst usually occurs in first two decades of life and has slight female preponderance as compared to male [2]. The exact etiology and pathogenesis of aneurysmal bone cyst is still not yet well defined. Lichtenstein [3] suggested that the aneurysmal bone cyst arises due to a persistent local disturbance in hemodynamics (venous thromboses or arteriovenous aneurysm) and causes marked increase in venous pressure which leads to the development of a dilated engorged vascular bed. There are also some evidence given by some authors in the scientific journals that aneurysmal bone cysts arise on a preexisting bone lesion as a secondary reaction [4, 5]. Trauma has been implicated as an initiative factor in some cases due to the fact that aneurysmal bone cyst is preceded by trauma with fracture or subperiosteal hematoma [6]. However, most of the authors agree that trauma draws attention to a preexisting lesion [7,8]. Now, the genetic basis of aneurysmal bone cyst has also been investigated, and specific chromosomal translocations have been reported [9,10,11]. It is also postulated that over expression of insulin-like growth factor 1 plays a role in the pathogenesis [11,12]. There are four radiological stages of aneurysmal cyst as described in the literature as: Initial, active, stabilization, and healing [13]. In the initial phase, the lesion is characterized by a well-defined area of osteolysis with a discrete elevation of the periosteum. This is followed by a growth phase, in which the lesion grows rapidly with progressive destruction of bone and development of the characteristic blown-out radiologic appearance. Then, there is the stage of stabilization, in which the characteristic soap bubble appearance develops as a result of maturation of the bony shell. Diagnosis generally occurs during the active or stabilization phase. Final healing results in progressive calcification and ossification, with the lesion transformed into a dense bony mass. Aneurysmal bone cyst histologically composed of cavernous or slit-like hemorrhagic spaces surrounded and traversed by fibrous septa containing spindled cells, inflammatory cells. Rarely, lesser number of osteoclast-like multinucleated giant cells can be seen which are often distributed around the hemorrhagic, cystic spaces. Typically, osteoid formation with or without osteoblastic rimming is observed as a typical feature [11,14]. Although, various options for the treatment of aneurysmal bone cyst have been reported in the literature [15], controversy exists regarding optimal treatment. Due to its rarity in the hand, there is no established evidence-based treatment regimen. We here report a case of aneurysmal bone cyst of 3rd metacarpal, managed with resection and bone grafting and later followed.
Case report
A 13-year-old young female presented with pain and progressive increase in swelling over the dorsum of the right hand for 7–8 months. There was pain and tenderness over 3rd metacarpal. There was painful restriction of movement at the metacarpophalangeal joints. There was no history of trauma, fever, loss of weight, or loss of appetite. The patient also was having slight difficulty in making fist. Skin was normal and temperature was not raised. Distal neurovascular structures were intact. Serial radiographic evaluation of the hand from May 2009 to October 2010 showed multilocular expansile lytic lesion with ballooning of 3rd metacarpal with increasing size. There was a widening of medullary canal and thinning of cortex with pathological fracture (Fig. 1).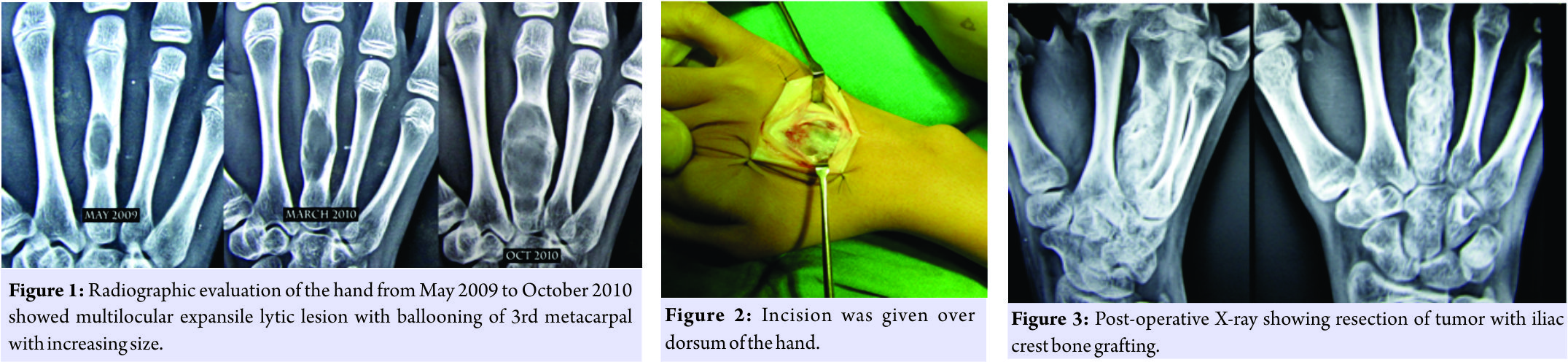 The patient was managed surgically. Incision was given over dorsum of the hand (Fig. 2). Resection with curettage of tumor was done, and the void was filled by iliac crest bone graft (Fig. 3). Sample was sent for histopathological examination. Histopathology section suggested fibrous septa enclosing hemorrhagic cystic space. Septa contained bony chips, spindle cell, inflammatory cell, and few scattered osteoclast. There was no sign of malignancy and diagnosis of aneurysmal bone cyst of 3rd metacarpal was made.
The patient was managed surgically. Incision was given over dorsum of the hand (Fig. 2). Resection with curettage of tumor was done, and the void was filled by iliac crest bone graft (Fig. 3). Sample was sent for histopathological examination. Histopathology section suggested fibrous septa enclosing hemorrhagic cystic space. Septa contained bony chips, spindle cell, inflammatory cell, and few scattered osteoclast. There was no sign of malignancy and diagnosis of aneurysmal bone cyst of 3rd metacarpal was made.
Result
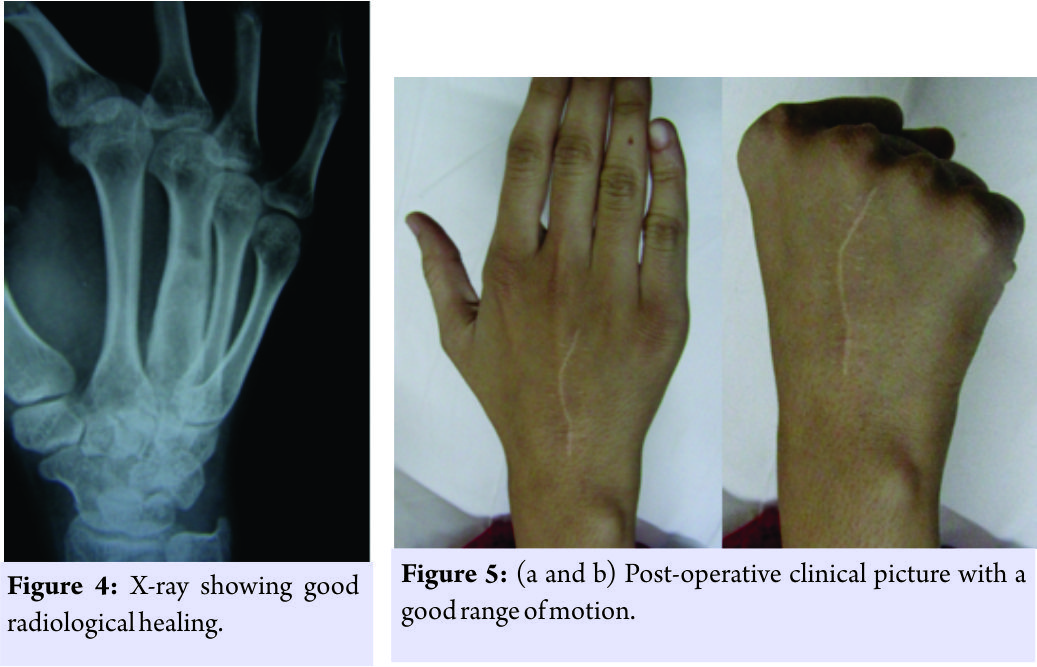
Postoperatively below elbow back, slab was applied and the patient was comfortable. On 2nd post-operative day onward, previous severe and continuous pain was relieved except for surgical site pain which was reducing gradually. At the day of suture removal on post-operative day 14, back slab was removed and the patient was absolutely pain free. The patient was followed up after 5 years. Good radiological healing was seen (Fig. 4). The patient is pain free and having a good range of motion, good grip strength without any recurrence (Fig. 5a and b).
Discussion
The goal of treatment is the eradication of the lesion and preservation of function without recurrence. Many treatment modalities have been reported in literature including radiation, curettage and bone grafting, cryotherapy, and excision. However, controversy exists in the literature regarding optimal treatment. Due to its rarity in the hand, no evidence-based treatment regimen has been established. According to Ropars et al. [16], it was suggested that curettage and grafting are sufficient for treatment, and aggressive methods such as cryotherapy or resection with reconstruction should only be used in case of recurrences and articular involvement. Other parallel successful outcomes have been reported by other authors in scientific literature with no relapse after simple curettage and grafting [17,18]. The limitation of this procedure is graft resorption by osteoclastic activity, and if graft incorporation occurs also, it may take years to remodel. Possible recurrence after insufficient primary treatment will increase the size of the defect and the tumor may reach joint structures, which may need consequent bone grafting to include the epiphysis and even complete joints. Curettage and bone grafting are the most common operative procedure, but recurrence rate is high. Basarir et al. [12] reported recurrence in two of three cases that were initially treated with curettage and grafting. Similarly, Frassica et al. [19] study showed recurrence in four cases out of seven after curettage and bone grafting. To decrease the rate of local recurrence, after curettage and grafting, various forms of adjunctive therapy have been used. In some cases, cryosurgery [11,20,21] and sclerotherapy were used as an adjuvant intralesional treatment for aneurysmal bone cyst arising in the hand. These treatments may damage surrounding intact tissue and cause serious complications such as infection, neuropraxia, post-operative fracture, and burn in hand. En bloc resection and reconstruction with strut grafting is another operative treatment option. It seems to be the therapy of choice. No recurrence has been reported after en bloc resection in the relevant literature [1,2,12]. In an experimental study, it has been shown that bone defects that are left empty heal just as well as when filled with a bone substitute and defect protection alone was sufficient to allow for healing even of critical size defects [22]. The remodeling and reconstitution of cavities with cortical thickening over time can give sufficient strength even without filling.
Conclusion
Aneurysmal bone cyst in metacarpal is a rare benign bone tumor that can grow rapidly. Diagnosis can be made with clinical and radiological examination. Controversy exists in the literature regarding optimal treatment. Due to its rarity in the hand, no evidence-based treatment regimen has been established. The patient can be managed surgically with curettage and bone grafting, and a good radiological healing, pain-free good range of motion, and good grip strength can be obtained with almost no recurrence.
Clinical Message
Of all discussed procedures, curettage of tumor mass with bone grafting is one of the safest procedures with good clinical outcome for aneurysmal bone cyst of 3rd metacarpal. Identifying the correct tumor margin and filling the void with adequate bone graft are the key factor for achieving success, and by this method, we can avoid hampering the adjacent joint function and nearby soft tissue complications.
References
1. Koskinen EV, Visuri TI, Holmstrom T, RoukkulaM AB. Evaluation of resection and of curettage in 20 cases. Clin Orthop 1976;118:136-46.
2. Kotwal PP, Jayaswal A, Singh MK, Dave PK. Aneurysmal bone cyst in the metacarpal of a child a case report. J Hand Surg Br 1988;13:479-80.
3. Lichtenstein L. Aneurysmal bone cyst; Further observations. Cancer 1953;6:1228-37.
4. Biesecker JL, Marcove RC, Huvos AG, Miké V. Aneurysmal bone cysts. A clinico-pathologic study of 66 cases. Cancer 1970;26:615-25.
5. Buraczewski J, Dabska M. Pathogenesis of aneurysmal bone cyst. Relationship between the aneurysmal bone cyst and fibrous dyspla-sia of bone. Cancer 1971;28:597-604.
6. Dabezies EJ, D’Ambrosia RD, Chuinard RG, Ferguson AB Jr. Aneurysmal bone cyst after fracture. A report of three cases. J Bone Joint Surg Am 1982;64:617-21.
7. Fuhs SE, Herndon JH. Aneurysmal bone cyst involving the hand: A review and report of two cases. J Hand Surg Am 1979;4:152-9.
8. Burkhalter WE, Schroeder FC, Eversmann WW Jr. Aneurysmal bone cysts occurring in the metacarpals: A report of three cases. J Hand Surg Am 1978;3:579-84.
9. Panoutsakopoulos G, Pandis N, Kyriazoglou I, Gustafson P, Mertens F, Mandahl N, et al. Recurrent t(16;17)(q22;p13) in aneurysmal bone cysts. Genes Chromosomes Cancer 1999;26:265-6.
10. Oliveira AM, Hsi BL, Weremowicz S, Rosenberg AE, Dal Cin P, Joseph N, et al. USP6 (Tre2) fusion oncogenes in aneurysmal bone cyst. Cancer Res 2004;64:1920-3.
11. Mendenhall WM, Zlotecki RA, Gibbs CP, Reith JD, Scarborough MT, Mendenhall NP. Aneurysmal bone cyst. Am J Clin Oncol 2006;29:311-5.
12. Leithner A, Lang S, Windhager R, Leithner K, Karlic H, Kotz R, et al. Expression of insulin-like growth factor-I (IGF-I) in aneurysmal bone cyst. Mod Pathol 2001;14:1100-4.
13. Dabska M, Buraczewski J. Aneurysmal bone cyst. Pathology, clinical course and radiologic appearances. Cancer 1969;23:371-89.
14. Martinez V, Sissons HA. Aneurysmal bone cyst. A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61:2291-304.
15. Cottalorda J, Bourelle S. Modern concepts of primary aneurysmal bone cyst. Arch Orthop Trauma Surg 2007;127:105-14.
16. Ropars M, Kaila R, Briggs T, Cannon S. An eurysmal bone cysts of the metacarpals and phalanges of the hand. A 6 case series and literature review [in French]. Chir Main 2007;26:214-7.
17. Sakka SA, Lock M. Aneurysmal bone cyst of the terminal phalanx of the thumb in a child. Arch Orthop Trauma Surg 1997;116:119-20.
18. Sproule JA, Salmo E, Mortimer G, O’Sullivan M. Aneursymal bone cyst of the proximal phalanx of the thumb in a child. Hand Surg 2002;7:147-50.
19. Leithner A, Windhager R, Lang S, Haas OA, Kainberger F, Kotz R, et al. Aneurysmal bone cyst. A population based epidemiologic study and literature review. Clin Orthop Relat Res 1999;363:176-9.
20. Ruiter DJ, van Ryssel TH, vander Velde EA. ABC a clinicopathological study of 105 cases. Cancer 1977;39:2231-9.
21. Schreuder HW, Veth RP, Pruszczynski M, Lemmens JA, Koops HS, Molenaar WM, et al. Aneurysmal bone cysts treated by curettage, cryotherapy and bone grafting. J Bone Joint Surg Br 1997;79:20-5.
22. Lemperle SM, Calhoun CJ, Curran RW, Holmes RE. Bony healing of large cranial and mandibular defects protected from soft-tissue interposition: A comparative study of spontaneous bone regeneration, osteoconduction, and cancellous autografting in dogs. Plast Reconstr Surg 1998;101:660-72.
 |
 |
 |
 |
| Dr. Saurav Narayan Nanda | Dr. Sanjay Tripathi | Dr. Shaikh Muzammil Shiraz | Dr. Sudhir Warrier |
| How to Cite This Article: Nanda S N, Tripathi S, Shiraz S M, Warrier S. Aneurysmal Bone Cyst of 3rd Metacarpal, Management and Follow-up: A Case Report. Journal of Orthopaedic Case Reports 2018 Mar- April; 8(2): 9-12. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


